
“History is written by the victors”
Sir Winston Churchill
It is some achievement if we can be acknowledged as succeeding in our field of work. If that field of work happens to be helping to win the most bloody conflict in history then our achievement deserves legendary status. What then do you say of a man who not only succeeded in his field and helped the Allies win the Second World War but whose work continues to resonate throughout life today? Abraham Wald was a statistician whose unique insight echoes in areas as diverse as clinical research, finance and the modern celebrity obsession. This is his story and the story of survivorship bias. This is the story of why we must take a step back and think.
Abraham Wald and Bullet Holes in Planes
Wald was born in 1902 in the then Austria-Hungarian empire. After graduating in Mathematics he lectured in Economics in Vienna. As a Jew following the Anschluss between Nazi Germany and Austria in 1938 Wald and his family faced persecution and so they emigrated to the USA after he was offered a university position at Yale. During World War Two Wald was a member of the Statistical Research Group (SRG) as the US tried to approach military problems with research methodology.
One problem the US military faced was how to reduce aircraft casualties. They researched the damage received to their planes returning from conflict. By mapping out damage they found their planes were receiving most bullet holes to the wings and tail. The engine was spared.
DISTRIBUTION OF BULLET HOLES IN AIRCRAFT THAT RETURNED TO BASE AFTER MISSIONS. SKETCH BY WALD. IN “VISUAL REVELATIONS” BY HOWARD WAINER. LAWRENCE ERLBAUM AND ASSOCIATES, 1997.
Abraham Wald
The US military’s conclusion was simple: the wings and tail are obviously vulnerable to receiving bullets. We need to increase armour to these areas. Wald stepped in. His conclusion was surprising: don’t armour the wings and tail. Armour the engine.
Wald’s insight and reasoning was based on understanding what we now call survivorship bias. Bias is any factor in the research process which skews the results. Survivorship bias describes the error of looking only at subjects who’ve reached a certain point without considering the (often invisible) subjects who haven’t. In the case of the US military they were only studying the planes which had returned to base following conflict i.e. the survivors. In other words what their diagram of bullet holes actually showed was the areas their planes could sustain damage and still be able to fly and bring their pilots home.
No matter what you’re studying if you’re only looking at the results you want and not the whole then you’re subject to survivorship bias.
Wald surmised that it was actually the engines which were vulnerable: if these were hit the plane and its pilot went down and didn’t return to base to be counted in the research. The military listened and armoured the engine not the wings and tail.
The US Airforce suffered over 88,000 casualties during the Second World War. Without Wald’s research this undoubtedly would have been higher. But his insight continues to this day and has become an issue in clinical research, financial markets and the people we choose to look up to.
Survivorship Bias in Clinical Research
In 2010 in Boston, Massachusetts a trial was conducted at Harvard Medical School and Beth Israel Deaconess Medical Center (BIDMC) into improving patient survival following trauma. A major problem following trauma is if the patient develops abnormal blood clotting or coagulopathy. This hinders them in stemming any bleeding they have and increases their chances of bleeding to death. Within our blood are naturally occurring proteins called factors which act to encourage blood clotting. The team at Harvard and BIDMC investigated whether giving trauma patients one of these factors would improve survival. The study was aimed at patients who had received 4-8 blood transfusions within 12 hours of their injury. They hoped to recruit 1502 patients but abandoned the trial after recruiting only 573.
Why? Survivorship bias. The trial only included patients who survived their initial accident and then received care in the Emergency Department before going to Intensive Care with enough time passed to have been given at least 4 bags of blood. Those patients who died prior to hospital or in the Emergency Department were not included. The team concluded that due to rising standards in emergency care it was actually very difficult to find patients suitable for the trial. It was therefore pointless to continue with the research.
This research was not the only piece reporting survivorship bias in trauma research. Does this matter? Yes. Trauma is the biggest cause of death worldwide in the under 45 year-olds. About 5.8 million people die worldwide due to trauma. That’s more than the annual total of deaths due to malaria, tuberculosis and HIV/AIDS. Combined. Or, to put it another way, one third of the total number of deaths in combat during the whole of the Second World War. Every year. Anything that impedes research into trauma has to be understood. Otherwise it costs lives. But 90% of injury deaths occur in less economically developed countries. Yet we perform research in Major Trauma Units in the West. Survivorship bias again.
As our understanding of survivorship bias grows so we are realising that no area of Medicine is safe. It clouds outcomes in surgery and anti-microbial research. It touches cancer research. Cancer survival rates are usually expressed as 5 year survival; the percentage of patients alive 5 years after survival. But this doesn’t include the patients who died of something other than cancer and so may be falsely optimistic. However, Medicine is only a part of the human experience survivorship bias touches.
Survivorship Bias in Financial Markets & our Role Models
Between 1950 and 1980 Mexico industrialised at an amazing rate achieving an average of 6.5% growth annually. The ‘Mexico Miracle’ was held up as an example of how to run an economy as well as encouraging investment into Latin American markets. However, since 1980 the miracle has run out and never returned. Again, looking only at the successes and not the failures can cost investors a lot of money.
Say I’m a fund manager and I approach you asking for investment. I quote an average of 1.8% growth across my funds. Sensibly you do your research and request my full portfolio:
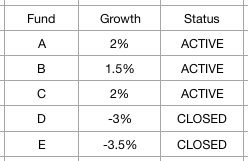
It is common practice in the fund market to only quote active funds. Poorly performing funds, especially those with negative growth, are closed. If we only look at my active funds in this example then yes, my average growth is 1.8%. You might invest in me. If however you look at all of my portfolio then actually my average performance is -0.2% growth. You probably wouldn’t invest then.
Yet survivorship bias has a slight less tangible effect on modern life now. How often is Mark Zuckerberg held up as an example for anyone working in business? We focus on the one self-made billionaire who dropped out of education before making their fortune and not the thousands who followed the same path but failed. A single actor or sports star is used as a case study on how to succeed and we are encouraged to follow their path never mind that many who do fail. Think as well about how we look at other aspects of life. How often do we look at one car still in use after 50 years or one building still standing after centuries and say, “we don’t make them like they used to”? We overlook how many cars or buildings of a similar age have now rusted or crumbled away. All of this is the same thought process going through the minds of the US Military as they counted bullet holes in their planes.
To the victor belong the spoils but we must always remember the danger of only looking at the positive outcomes and ignoring those often invisible negatives. We must be aware of the need to see the whole picture and notice when we are not. With our appreciation of survivorship bias must also come an appreciation of Abraham Wald. A man whose simple yet profound insight shows us the value of stepping back and thinking.
Thanks for reading
- Jamie


